Introduction
Intestinal capillariasis was first observed in the Philippines in 1962 and since then it has been noted, although less frequently in Thailand, with scattered reports from Taiwan, Japan, Egypt, and Iran. Capillaria Philippinensis is a small nematode which burrows into the intestinal mucosa of its human host. Humans and birds become infected when they eat uncooked or poorly cooked fish. Therefore, infections are seen in endemic proportions where uncooked fish is considered a delicacy.
Life Cycle
The complete life cycle is not known however, human infection is initiated by the consumption of raw fish. The infective larvae are found in the intestine of the fish. When infective fish are eaten by humans, the larvae mature and the adult worms live in the intestinal mucosa, mainly in the jejunum, where they are usually present in large numbers. Larval stages, oviparous and larviparous females are also found in the host’s intestine, which suggests that the nematode multiplies in the intestine resulting in auto-infection as in Strongyloides infection. The eggs are passed out in the feces and embryonate in the soil, a process which takes about 12 days. The eggs are ingested by fresh-water fish, they hatch and develop into the infective form in the intestine of the fish.
Life cycle of Capillaria philippinensis
Morphology
The adult female worm measures 2.5-4.3mm, while the males are marginally smaller measuring 2.3-3.2mm. Adult females can produce immature and mature ova as well as free larvae that can auto-infect. The eggs measure 45μm x 21μm, and resemble those of Trichuris but have less prominent polar plugs. They have a thick striated shell.

Capillaria philippinensis adult female worm

Capillaria philippinensis, male

Capillaria philippinensis male spicule

Capillaria philippinensis egg

Capillaria Philippinensis ova
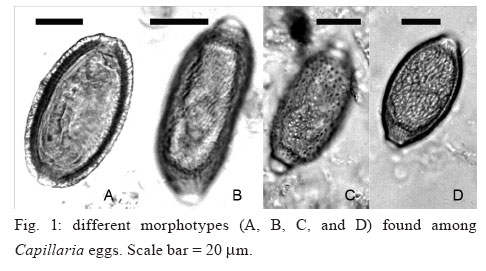
Capillaria philippinensis egg morphology

Autopsy specimen of human intestine showing numerous sections of C. philippinensis (arrows) and debris.

larvae of Capillaria philippinensis
Clinical Disease
Many cases may be asymptomatic, but any manifested symptoms will be related to the worm burden. The most common symptoms are watery stools with large fluid loss, anorexia, nausea, vomiting, and hypotension. Abdominal distension and edema may also develop. Death can ensue from pneumonia, cerebral edema, hypokalemia and heart failure. The large worm burden can cause electrolyte imbalance, plasma protein imbalance, and fluid loss, proving fatal within 4–6 months if untreated. Villi blunting leads to malabsorption but eosinophilia is not a feature of this disease.
Laboratory Diagnosis
Diagnosis depends on finding the characteristic eggs or larvae in the feces. Pulmonary capillariasis diagnosis relies on finding adult worms or eggs in lung biopsies.